
VH Bio’s HLA Technical Specialist, Ben Adams, describes the benefits and clinical utility of FLOWDSA-XM™ – a Flow Cytometry based crossmatch assay optimised for the detection of leukocyte antibodies.
Solid organ transplantation has continued to be supported by the development of novel histocompatibility methods since Patel and Terasaki described the significance of the positive crossmatch test in 1969. Subsequent innovations include development of the flow cytometry crossmatch (FCXM) in the 1980s, and bead-based multiplex assays for antibody detection in the 2000s.
In many laboratories, the FCXM has become the gold standard for crossmatching: offering sensitivity superior to the cytotoxic crossmatch. However, poor FCXM specificity in unsensitised or moderately sensitised patients means that some laboratories only utilise this methodology in a selected cohort of patients (e.g. those who are highly sensitised) where the false positive rate is lower.
The One Lambda FlowDSA-XM™ 1 2 3 offers an additional tool to the HLA laboratory by ensuring only HLA-specific antibodies are detected in the FCXM assay, thus bridging the gap between sensitive and specific antibody detection methods and the transplant-specific crossmatch intended to confirm the absence of donor-directed alloantibodies.
FlowDSA-XM™
The FlowDSA-XM™ method parallels the FCXM assay (Figure 1). Patient serum is incubated with donor lymphocytes, the cells are washed, and Capture Beads are added. A Lysis/Stain Buffer is added and Capture Beads bind donor HLA whilst donor-specific antibodies bound to HLA-Capture Bead complexes are ‘stained’ via Phycoerythrin-conjugated anti-human IgG. Following an additional wash, HLA-Bead complexes are ready for reading on a flow cytometer.
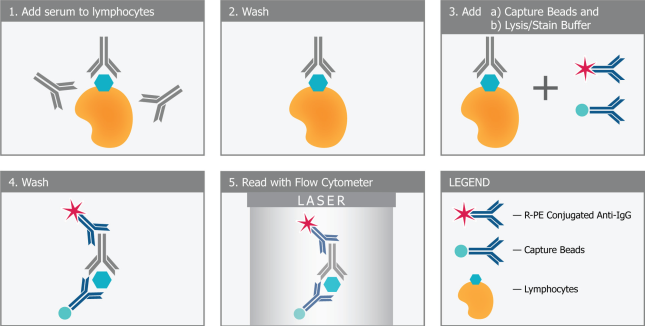
Figure 1: Principle of the FlowDSA-XM™.
FlowDSA-XM Capture Beads separate into three discrete populations: one representing HLA class I, and two representing HLA class II (Figure 2).
Gating on these bead populations allows the discrimination of HLA class I and class II reactivity, as indicated by a channel shift relative to the negative control and with fluorescence indicating the relative amount of HLA-specific antibody present.
Flow cytometer setup is straightforward, with FlowDSA-XM Capture Beads being used to establish the gains and compensation necessary for bead identification. The Positive/Negative Cut-off is established locally by replicate testing of AB male sera against different target cells.
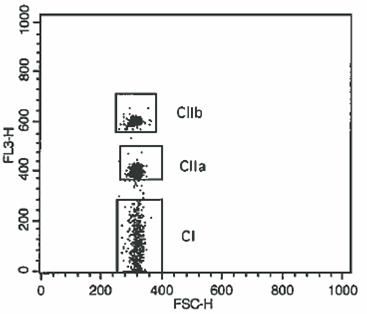
Figure 2: FlowDSA-XM™ selectively detects HLA-specific antibodies and allows the discrimination of HLA class I and class II antibodies.
Key benefits and clinical utility
FlowDSA-XM™ builds on the sensitivity of the FCXM and ability to detect non-complement fixing antibodies by improving specificity through the selective detection of HLA-specific antibodies.
The workflow is familiar and the length of testing similar to the standard FCXM. Fresh or frozen lymphocytes from various sources (e.g. peripheral blood, spleen) can be used, and implementing the FlowDSA-XM™ ought to require no capital investment for laboratories already undertaking crossmatching by flow cytometry.
Despite robust antibody definition strategies, HLA laboratories experience positive crossmatches for reasons that may or may not be explained. In a relatively liberal transplant centre an unexplained positive crossmatch might be interpreted as negative based upon recent or peri-transplant antibody screening, but with an acknowledgement of increased ‘risk’ and dependent on the degree of channel shift. In a more conservative transplant centre, the same situation could result in the patient being denied a transplant.
In permitting the transplant, unexplained reactivity is often explained by non-HLA or autologous antibodies. Hyperactive immunity may occur in specific disease groups (e.g. patients with HIV or Type I diabetes) or following vaccination, infection and medical procedures (including dentistry). In denying the transplant, recent changes in the patient’s antibody profile and technical challenges in identifying antibody specificities (e.g. aberrant reactivity or antigens absent in screening assays) might be considered justification.
Various immunoglobulin-based drugs result in positive crossmatches. For example, Rituximab (anti-CD20) and Alemtuzumab (anti-CD52) cause B cell positive FCXM, or T and B cell positive FCXM respectively; the polyclonal therapies Thymoglobulin and Intravenous Immunoglobulin yield similar results. Communication of their administration will alert the laboratory to the expected results, but regardless, immunoglobulin-based drugs can obscure true positive or true negative results for a prolonged period.
FlowDSA-XM™ allows the HLA laboratory to specifically attribute a positive FCXM to HLA-specific antibodies, discounting non-HLA antibodies, autoantibodies and medication as agents causative of the positive FCXM, and allowing the laboratory to accurately risk assess the proposed transplant.
Whilst FlowDSA-XM™ could be implemented as a front-line method, FlowDSA-XM™ certainly lends itself to selected transplants. For example, within the living donor setting (where time pressures are less acute), FlowDSA-XM™ could be used following an unexpected positive crossmatch to confirm the absence of donor-directed HLA-specific antibodies, potentially facilitating multiple transplants if involving Paired/Pooled Donation.
Additionally, FlowDSA-XM™ allows crossmatching up to the time of transplant and despite the use of induction agents in antibody incompatible transplantation (both HLAi and ABOi), allowing crossmatch outcome (negative, or limited channel shift) to be used as an endpoint in assessing the efficacy of desensitisation therapies. The utility of FlowDSA-XM™ in the clinical setting has already been demonstrated 4.
FlowDSA-XM™ is yet another tool offered by One Lambda to facilitate transplantation and support optimal outcomes. In addition to the HLA-specific LABScreen® 5 assays, LABScreen® Autoantibody joins the LABScreen® Mixed 6 7/MICA 8 9 (MICA) and Multi 10 11 (HNA) assays in identifying non-HLA antibody targets. One Lambda also offer AT1R and ETAR ELISAs 12 13 for the detection of anti-AT1R and -ETAR antibodies, and C1qScreen™ 14 15 for use alongside LABScreen® assays to allow the discrimination of complement-fixing antibodies.
Contact Ben to discuss this article or our HLA typing services, or speak to our sales team to learn more about FlowDSA-XM™.
References
- One Lambda FlowDSA-XM™. http://www.onelambda.com/en/products-services/products/antibody-detection/flowdsa-xm.html
- VHBio News: FlowDSA-XM™. https://vhbio.com/flowdsa-xm-new-one-lambda/
- VHBio Products: FlowDSA-XM™. https://vhbio.com/product/flowdsa-xm/
- One Lambda Webinar: Moving FCXM into the Future with FlowDSA-XM (Recorded 2017 Jun 22). http://www.onelambda.com/en/knowledge-support/Education/webinars.html
- One Lambda LABScreen®. http://www.onelambda.com/en/products-services/products/antibody-detection/labscreen.html
- One Lambda LABScreen® Mixed. http://www.onelambda.com/en/product/labscreen-mixed.html
- VHBio Products: LABScreen® Mixed. https://vhbio.com/product/labscreen-mixed-class-i-ii-antibody-screening/
- One Lambda LABScree® MICA. http://www.onelambda.com/en/product/labscreen-mica-1.html
- VHBio Products: LABScreen® MICA. https://vhbio.com/product/labscreen-mica-single-antigen-group-1/
- One Lambda LABScree® Multi. http://www.onelambda.com/en/product/labscreen-multi.html
- VHBio Products: LABScreen® Multi. https://vhbio.com/product/labscreen-multi/
- One Lambda AT1R and ETAR assays. http://www.onelambda.com/en/products-services/products/antibody-detection/at1r.html
- One Lambda C1qScreen™. http://www.onelambda.com/en/products-services/products/antibody-detection/c1q.html
- VHBio Products: C1qScreen™. https://vhbio.com/product/c1qscreen/
Enquire about this article
"*" indicates required fields